















Precision Diagnostic Services

Upper GI Endoscopy & Colonoscopy
Upper gastrointestinal endoscopy and colonoscopy are cornerstone procedures in modern gastroenterology, allowing direct visualization of the digestive tract for accurate diagnosis and timely treatment. Upper GI endoscopy evaluates the esophagus, stomach, and duodenum, while colonoscopy examines the colon and terminal ileum.
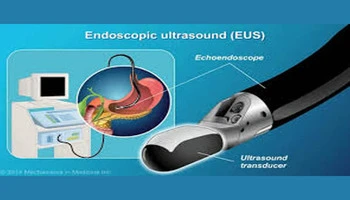
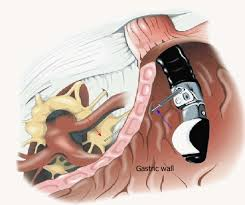
Endoscopic Ultrasonography (EUS)
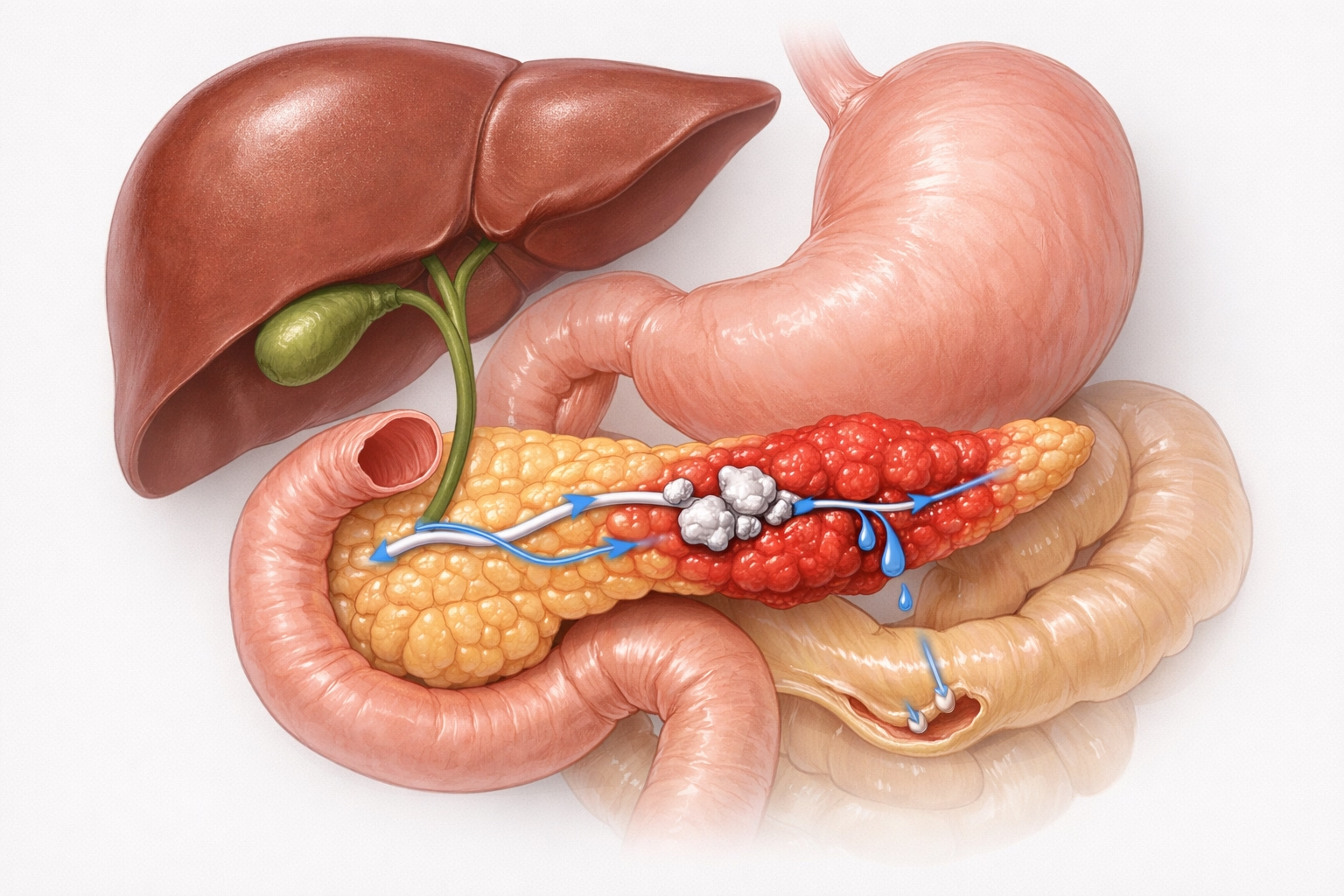
Endoscopic Ultrasonography (EUS) is an advanced imaging modality that combines endoscopy with high-frequency ultrasound to provide detailed visualization of the gastrointestinal wall layers and adjacent organs. It plays a critical role in evaluating pancreatic diseases, biliary disorders, submucosal tumors, lymph nodes, and mediastinal lesions that are difficult to assess with conventional imaging.

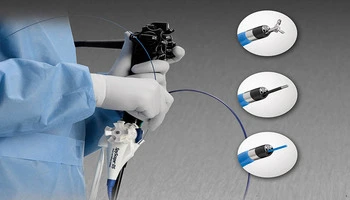
Fine Needle Aspiration (FNA) and Fine Needle Biopsy (FNB)
Fine Needle Aspiration (FNA) and Fine Needle Biopsy (FNB) allow accurate tissue diagnosis of pancreatic masses, lymph nodes, and deep-seated tumors with minimal risk.

Lumen-Apposing Metal Stents (LAMS)
Lumen-Apposing Metal Stents (LAMS) enable minimally invasive drainage of pancreatic pseudocysts and walled-off necrosis, avoiding open surgery.

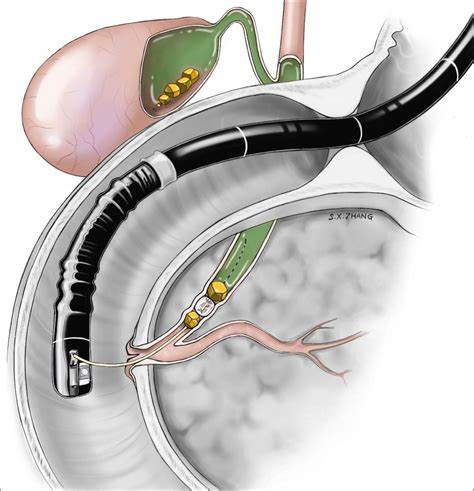
EUS-Guided Hepaticogastrostomy
EUS-Guided Hepaticogastrostomy, EUS guided choledochoduodenostomy and EUS guided cholecystogastrostomy provides internal biliary drainage when ERCP fails.
EUS-Guided Celiac Plexus Neurolysis
EUS-Guided Celiac Plexus Neurolysis offers effective pain relief in chronic pancreatitis and pancreatic cancer.
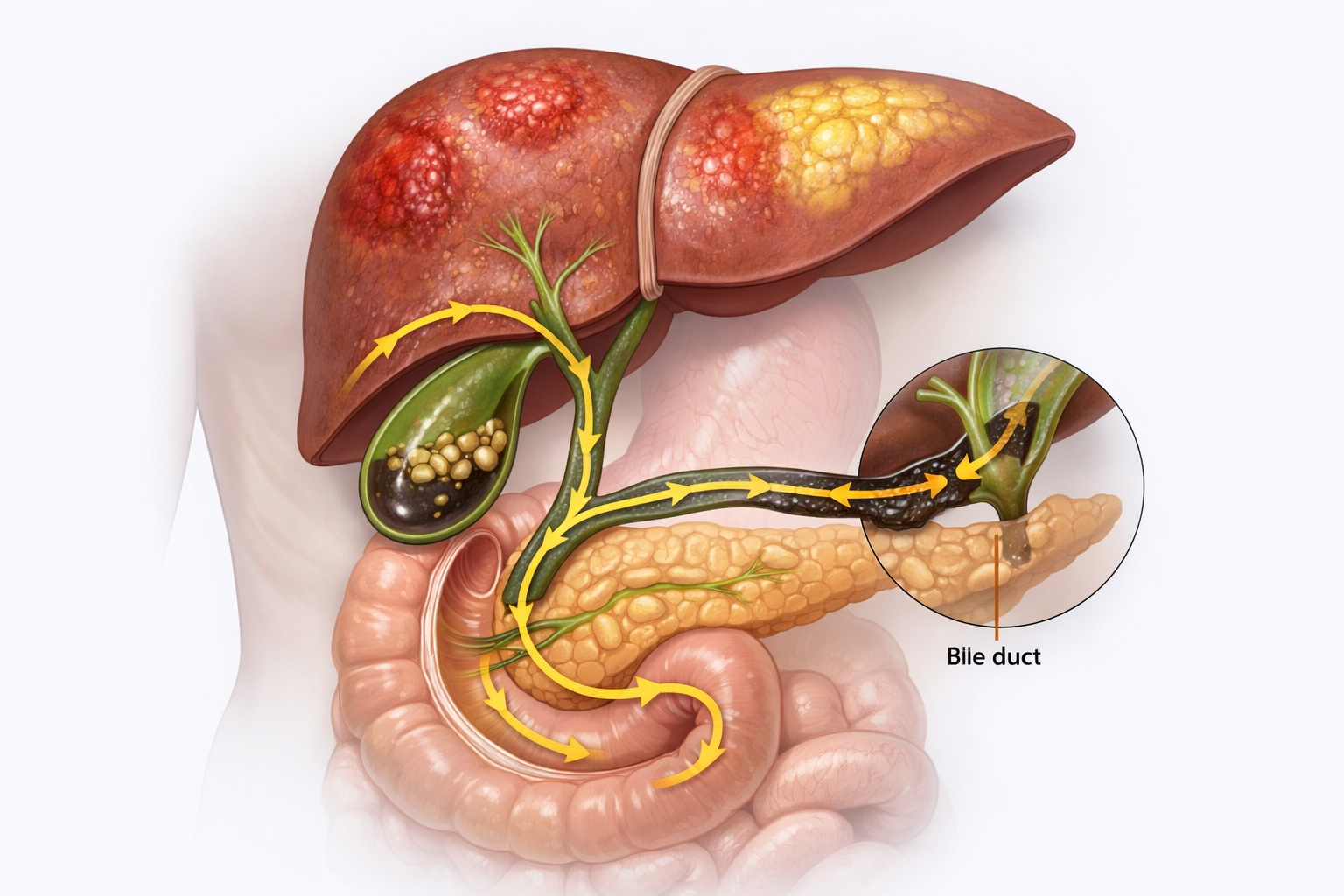
ERCP (Endoscopic Retrograde Cholangiopancreatography)
ERCP is a highly specialized endoscopic procedure used for the diagnosis and treatment of biliary and pancreatic duct disorders. It is commonly performed in patients with jaundice, cholangitis, bile duct stones, pancreatic duct strictures, and postoperative bile leaks.
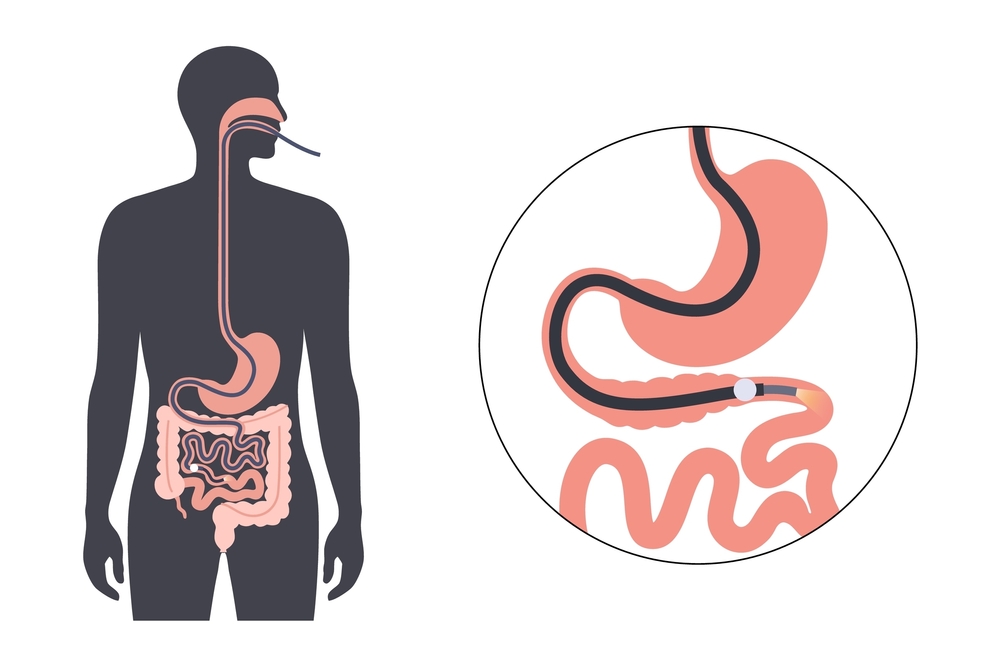
Single Balloon Enteroscopy
Single balloon enteroscopy is an advanced technique designed to evaluate and treat diseases of the small intestine, an area beyond the reach of routine endoscopy and colonoscopy. It is particularly valuable in patients with obscure gastrointestinal bleeding, unexplained iron-deficiency anemia, small bowel tumors, strictures, polyps, and angioectasias.
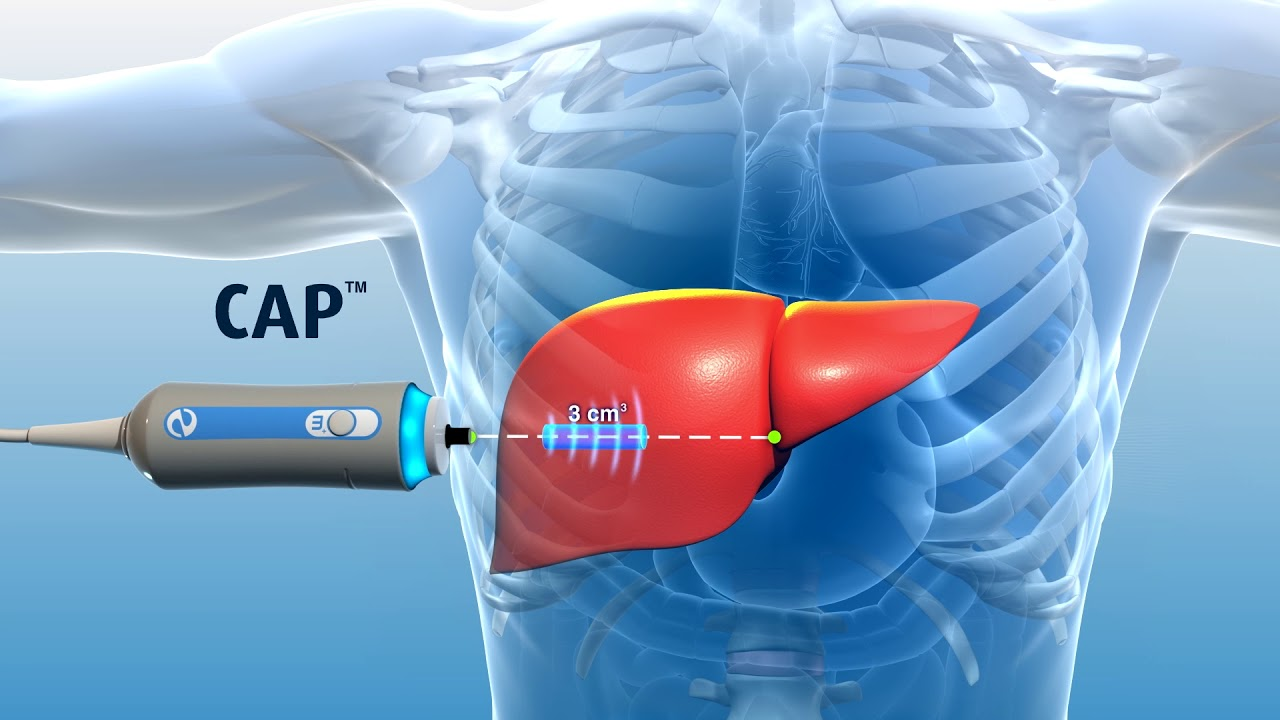
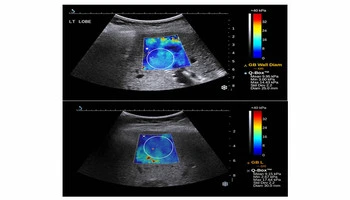
FibroScan & Shear Wave Elastography
FibroScan and Shear Wave Elastography are advanced, non-invasive imaging techniques used to assess liver stiffness and liver fat content, playing a crucial role in the evaluation and monitoring of chronic liver diseases. These technologies provide accurate quantification of liver fibrosis and steatosis without the need for invasive liver biopsy.
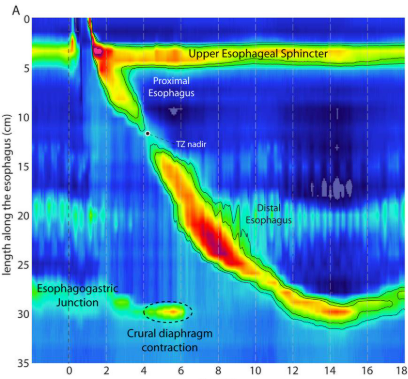
Esophageal & Anorectal Manometry, 24-hour pH Monitoring, Electrogastrography
Esophageal Manometry evaluates esophageal muscle contractions and lower esophageal sphincter function, playing a key role in diagnosing achalasia, diffuse esophageal spasm, and ineffective esophageal motility. This test is essential before anti-reflux surgery and POEM procedures.

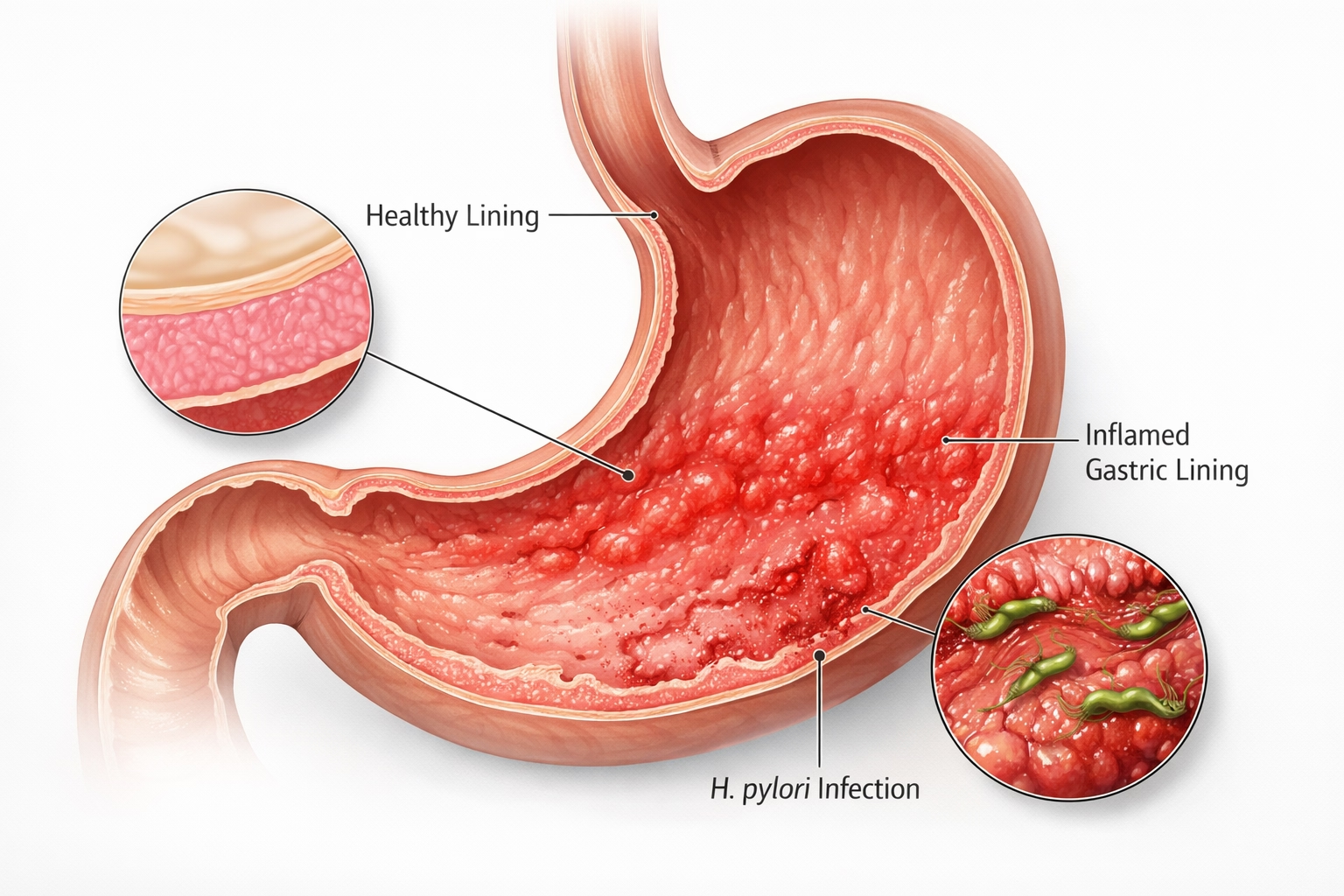
Breath Tests
Breath tests provide a simple, non-invasive method to diagnose specific gastrointestinal disorders related to infections and carbohydrate malabsorption. These tests are safe, painless, and highly reliable when performed under standardized protocols.
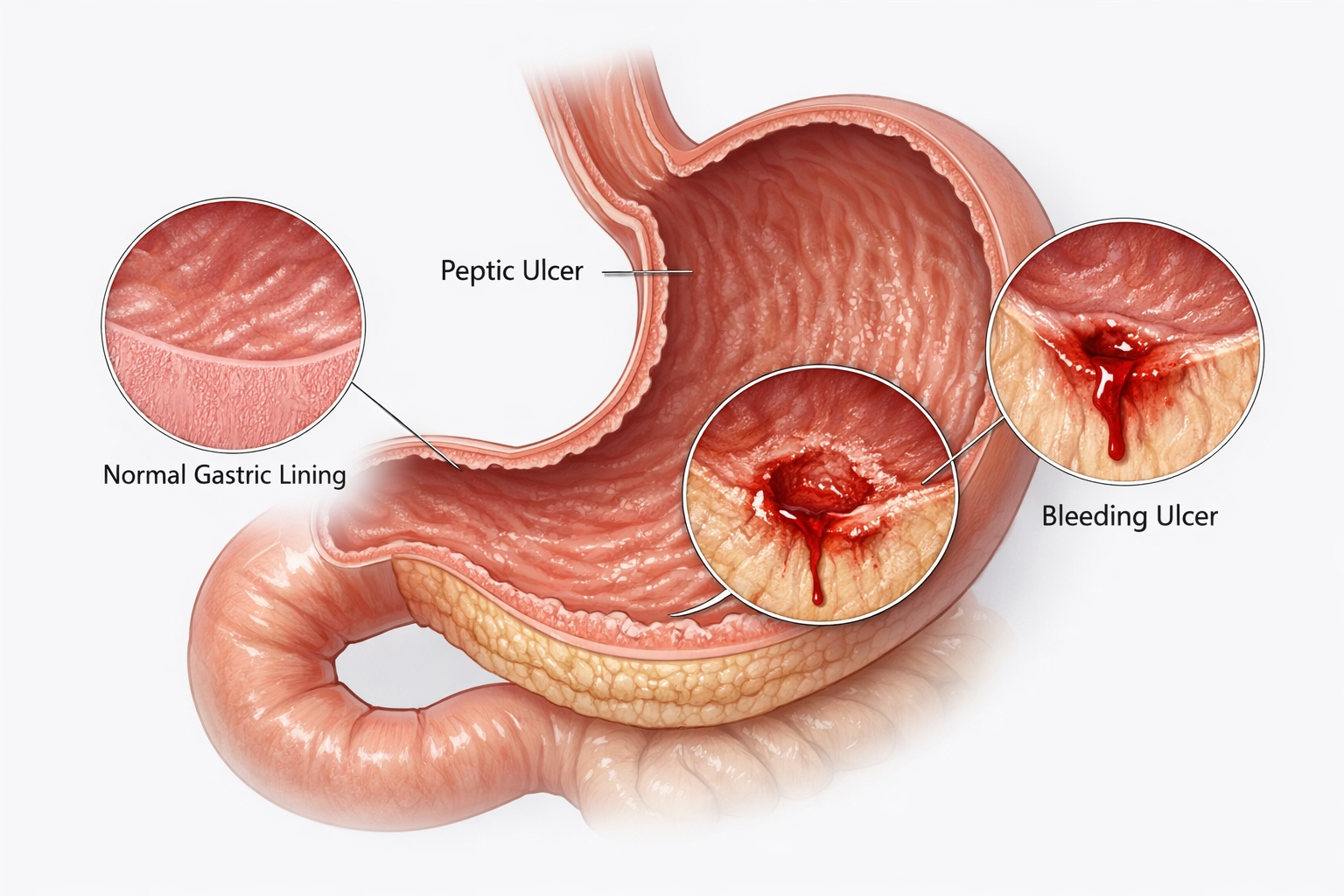
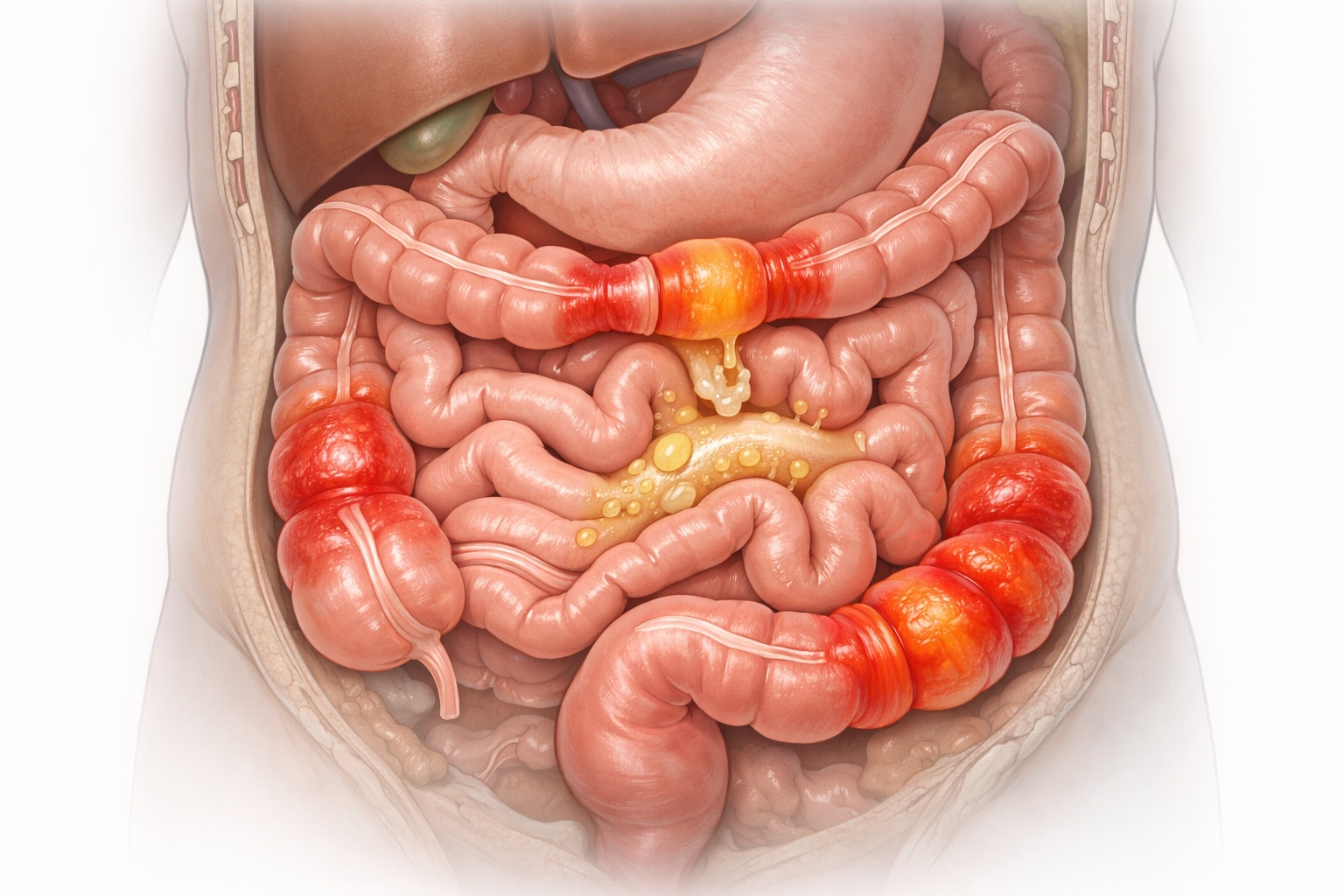
Gastrointestinal Bleeding Management
Endoscopic management of gastrointestinal bleeding is a life-saving intervention that allows rapid diagnosis and immediate treatment. Our center offers comprehensive endoscopic bleeding control for both upper and lower GI bleeding.
Biofeedback Therapy for Pelvic Floor & Defecation Disorders
Biofeedback therapy is a highly effective, non-invasive treatment offered to patients diagnosed with pelvic floor dysfunction after anorectal manometry testing. Many individuals with chronic constipation, difficulty in passing stools, or a sensation of incomplete evacuation have a condition known as dyssynergic defecation, where the pelvic floor muscles fail to relax appropriately during bowel movements.
Foreign Body & Gastrointestinal Stricture Management
Foreign body ingestion and gastrointestinal strictures can cause significant discomfort, obstruction, and serious complications if not treated promptly. Advanced endoscopic techniques allow safe, minimally invasive management without the need for open surgery in most cases.
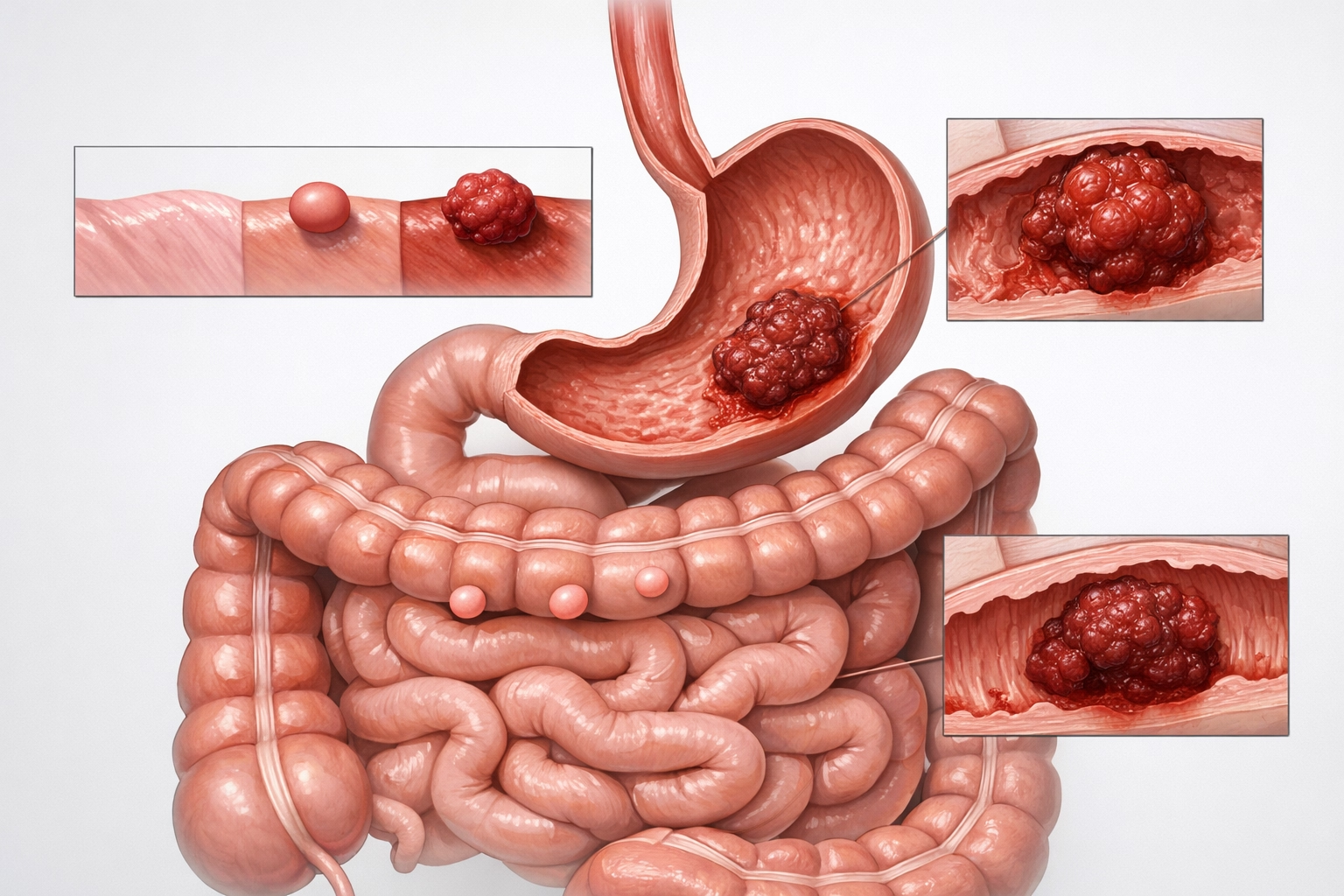
Tumor & Lesion Management
Early detection and minimally invasive treatment of gastrointestinal tumors and precancerous lesions are critical in preventing cancer progression and avoiding major surgery. Advanced endoscopic imaging and therapeutic techniques play a central role in modern GI oncology.
PEG & NJ Tube Insertions for Enteral Nutrition
Patients who are unable to consume adequate nutrition orally due to neurological disorders, malignancy, or prolonged critical illness benefit greatly from enteral feeding access. Percutaneous Endoscopic Gastrostomy (PEG) and Nasojejunal (NJ) tube placements provide safe and effective long-term nutritional support.
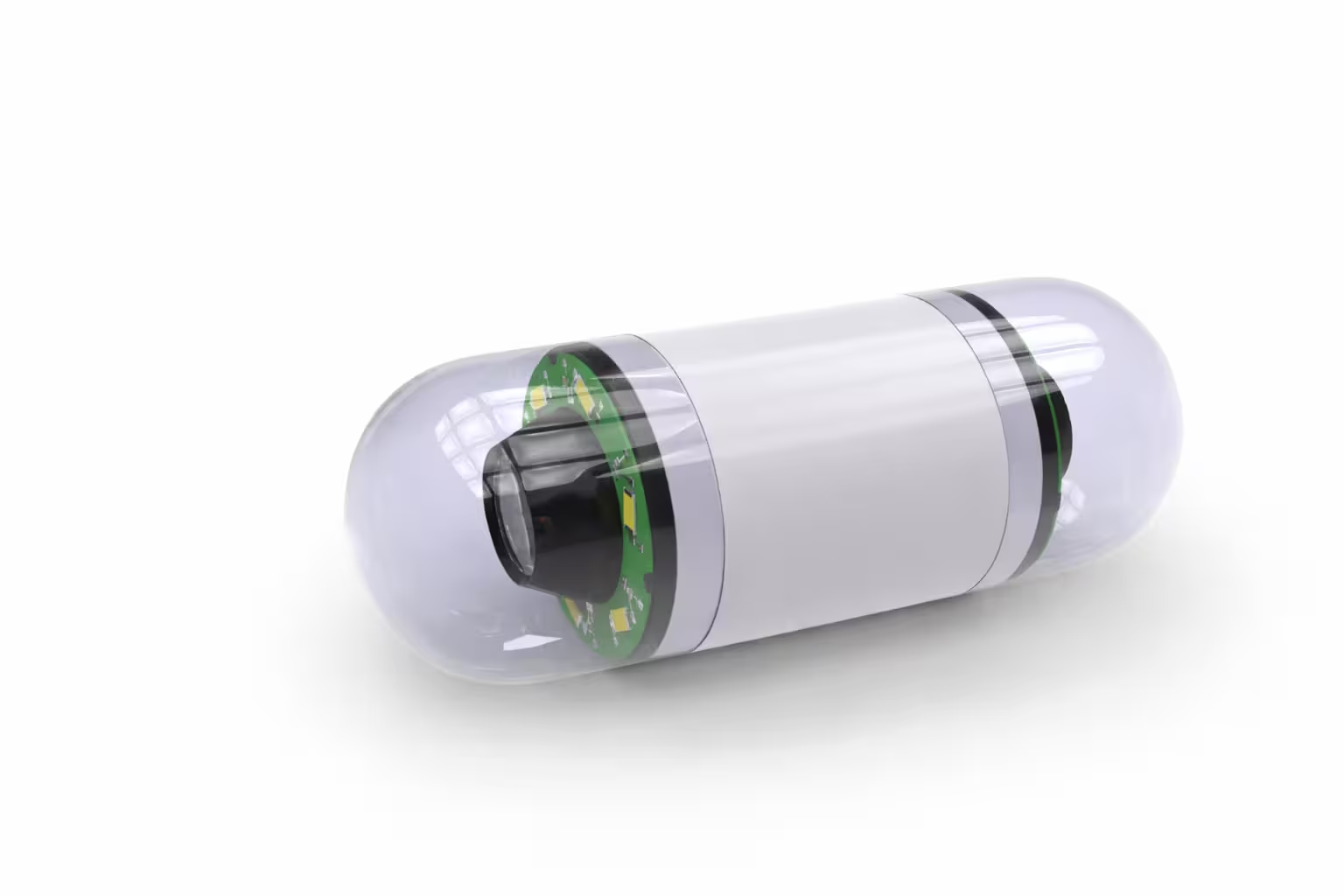
Capsule Endoscopy
Capsule endoscopy is a revolutionary, non-invasive technique that allows visualization of the entire small intestine, an area not easily accessible by conventional endoscopy or colonoscopy.The patient swallows a pill-sized capsule containing a miniature camera, light source, and transmitter.
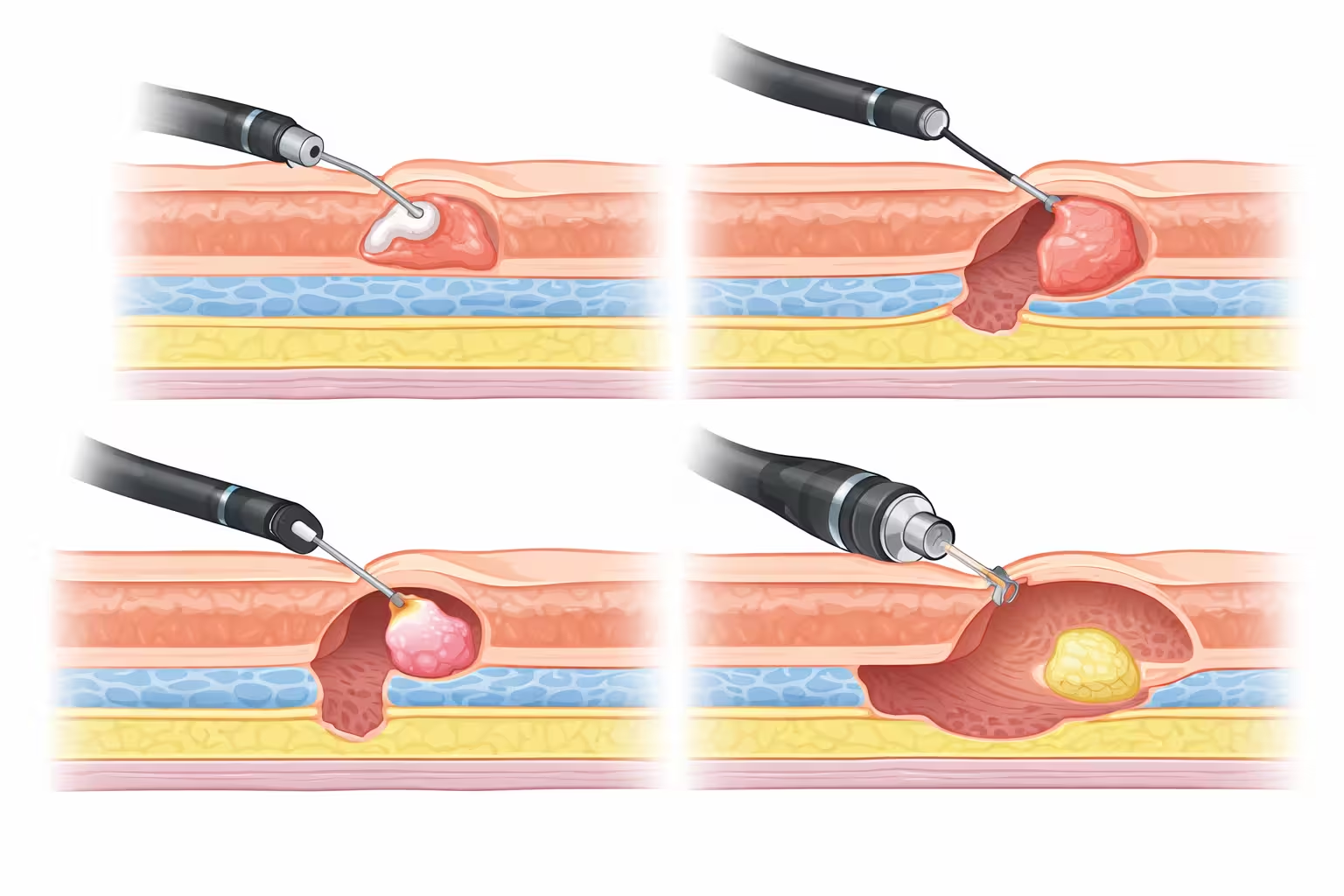
Third Space Endoscopy
Third space endoscopy represents a major advancement in minimally invasive gastrointestinal surgery, allowing complex lesions and motility disorders to be treated entirely through the endoscope without external incisions. These procedures target the "submucosal or third space" layer of the gastrointestinal tract, enabling precise and organ-preserving therapy.
POEM (Peroral Endoscopic Myotomy) for Achalasia
POEM is a state-of-the-art endoscopic procedure used to treat achalasia cardia and other esophageal motility disorders. Achalasia occurs when the lower esophageal sphincter fails to relax, leading to difficulty swallowing, chest pain, regurgitation, and weight loss.
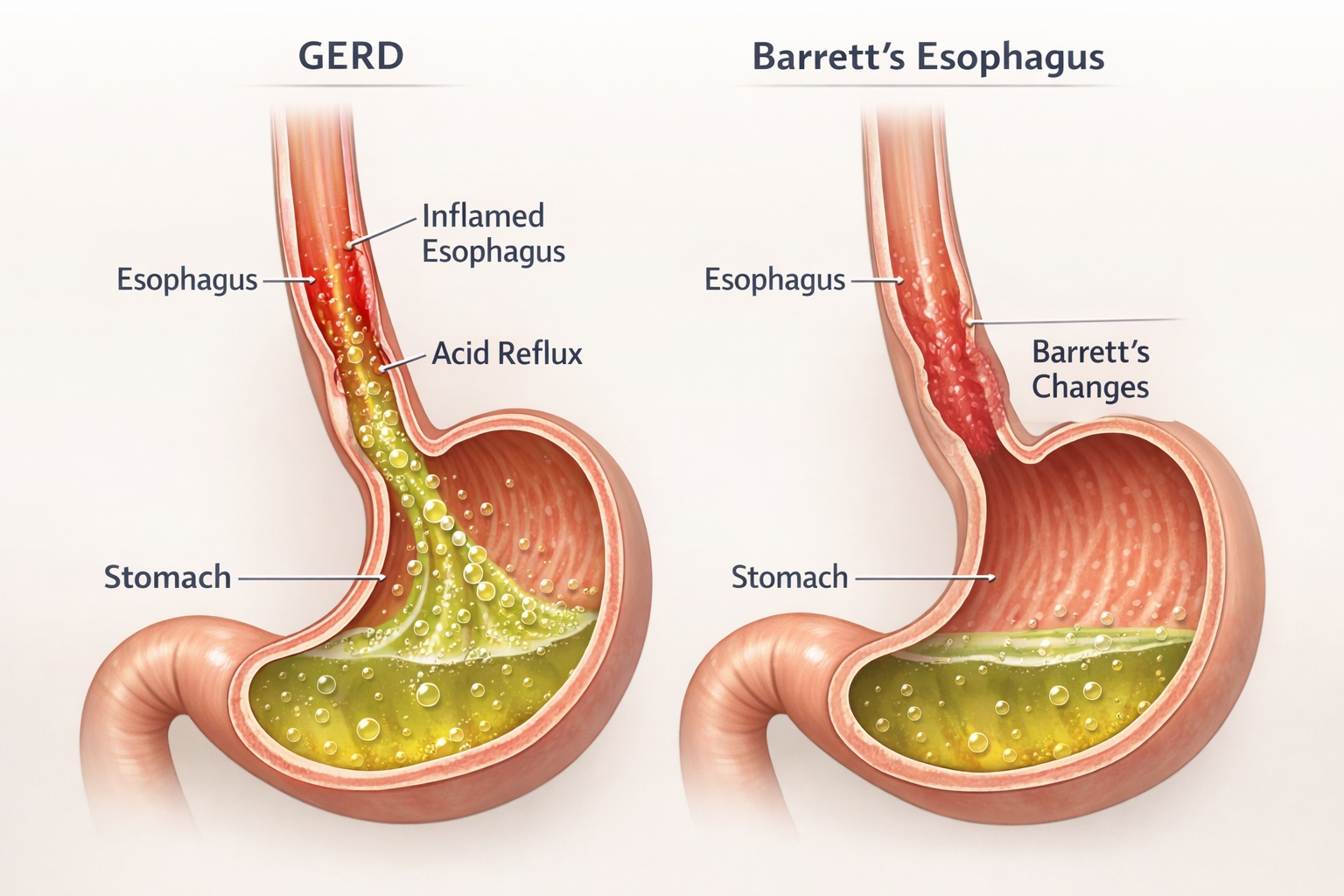
ARMS (Anti-Reflux Mucosectomy)
ARMS, or Anti-Reflux Mucosectomy, is an innovative endoscopic treatment for patients with gastroesophageal reflux disease (GERD) who do not respond adequately to medications. Unlike traditional anti-reflux surgery, ARMS is performed entirely through an endoscope without external cuts.
EUS-Guided Cholecystogastrostomy & Choledochoduodenostomy
EUS-guided biliary and gallbladder drainage procedures are advanced alternatives for patients in whom conventional ERCP is not feasible. These minimally invasive techniques provide internal drainage without the need for surgery or external tubes. EUS-guided cholecystogastrostomy involves creating a connection between the gallbladder and stomach using a lumen-apposing metal stent (LAMS).
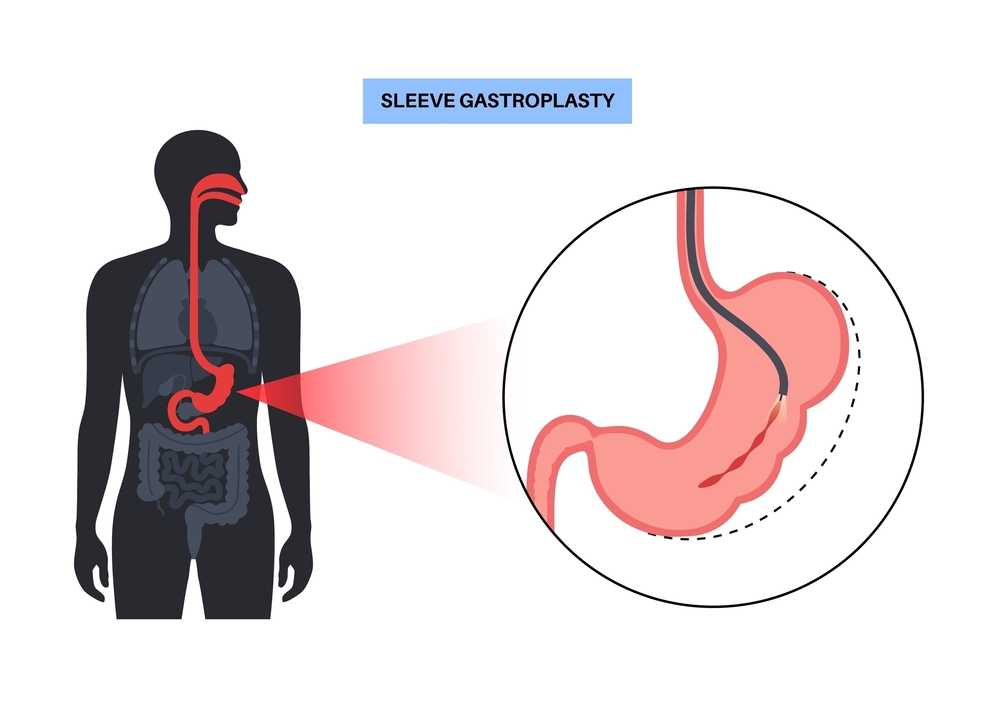
Obesity & Endobariatrics
Endobariatrics offers minimally invasive, endoscopic solutions for weight loss and metabolic improvement, providing effective alternatives to bariatric surgery.Endoscopic Sleeve Gastroplasty (ESG) reduces stomach volume using endoscopic suturing, promoting early satiety and sustained weight loss.